| |
| Bhigwan
(Pune District)
|
 |
|
|
|
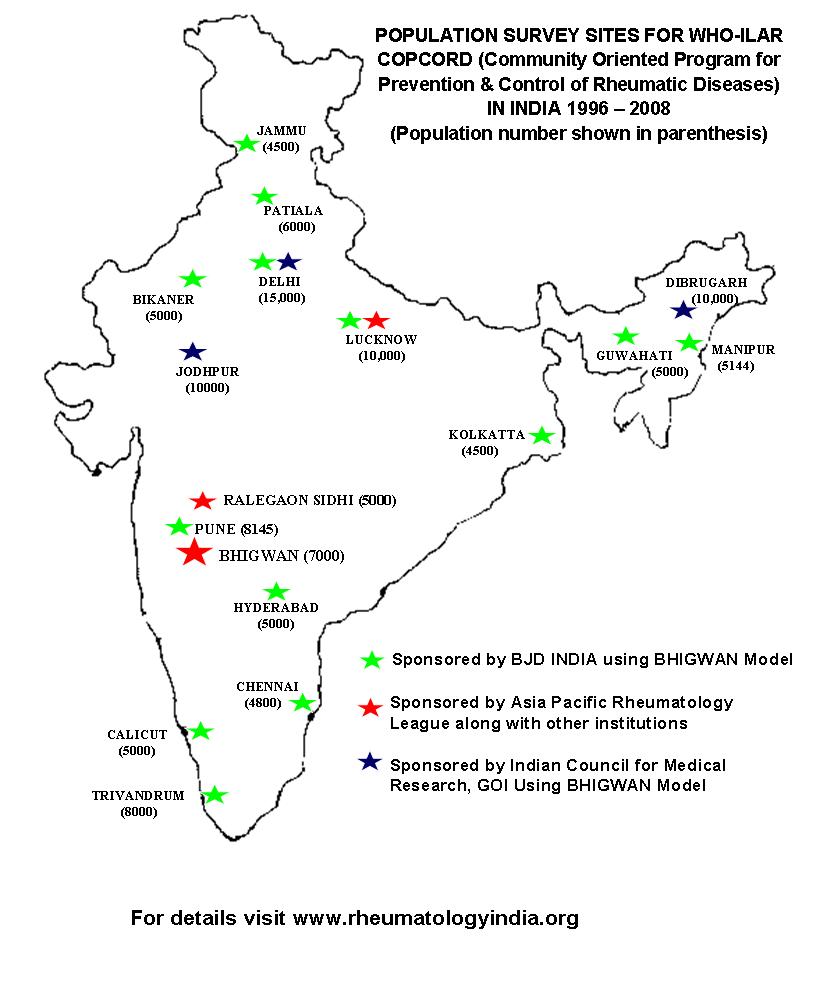
COPCORD
(Community Oriented Program for Control of Rheumatic
Diseases) is a global initiative of the WHO/International
League of Associations for Rheumatology (ILAR).
Under
the auspices of ILAR/APLAR, for the first time in
India, a COPCORD (Community Oriented Program for control
of rheumatic diseases) driven rural population survey
was carried out in Village Bhigwan (Pune District)
in 1996. The methodology used to extract information
is presented, along with some general results. In
Stage I Phase I, 6034 villagers (response rate 82%)
were screened in 16 days by 21 trained village volunteers.
Simultaneously, 774 patients (12.8%) identified completed
Phase 2 questionnaire (symptoms and disability) prior
to evaluation for diagnosis (Phase 3); limited laboratory
workup was carried out. The entire cross-sectional
survey was completed in 5 weeks. A pre-planned follow-up
program was begun essentially to verify the survey
diagnosis, identify new cases, impart health education
(Stage II), and attempt control of risk factors (Stage
III). A large community and patient data-base was
created. As per phase I answers, musculoskeletal/rheumatic
ailments were the commonest. The age and sex distribution
of “pain at any site” and “symptoms”
demonstrated preponderant problems in females, in
the age group 25-54 years. In almost one-third of
patients, a Symptom-Related-Diagnosis (34%) could
be offered while degenerative (29%) and soft-tissue
rheumatism disorders (20%) were commonly seen. Inflammatory
arthritis (11%), Rheumatoid arthritis (4%) in particular,
was seen in significant and unexpected proportions.
Well defined reactive arthritis, tropical forms of
arthritis (e.g. TB, Leprosy etc) and connective tissue
disorders were not evident.
The
Indian COPCORD study is a “fast-track-model”.
Unlike the previous COPCORD studies, this is an ongoing
long term longitudinal observational study, and is
in its tenth year running.
Using a similar model, a resurvey
was completed in 1999 – 2000 to validate
the initial survey
results.
The Bhigwan data
has been extensively presented
and published.
|
| |
| Pune |
|
|
| |
|
The
WHO – ILAR COPCORD Bhigwan (India) model has been
adopted for the ‘Population Based Multiregional
Urban Survey (2003-2004) for Rheumatic and other Musculoskeletal
Disorders’ study, Sponsored and funded by the
BJD-INDIA: NAN. The current model looks at several community
issues including quality of life, socio economic impact,
medical resources and health education.
The
urban study was begun in Jammu, Chennai and Pune in
April 2004. In, Pune, the survey has been completed
in the Narayan Peth locality in the heart of the city.
Over 9000 population has been surveyed and 888 patients
with different kinds of musculoskeletal rheumatic disorders
identified.
|
| |
|
|
A
rural population based study of Chikungunya infection
with special reference to persistent ‘rheumatic musculoskeletal
disorders
( An Indian Council of Medical Research, Govt. of India
sponsored project) |
Date of
commencement : September 2006
Date of completion : June 2008 |
| |
Chronic persistent
RMSK is the most important sequel of CHIKV that leads
to significant morbidity. In July-Sept 2006, several patients
of chronic RMSK following CHIKV were referred to CRD,
Pune, and the majority of these were inflammatory arthritis.
A wide spectrum of inflammatory arthritis, ranging from
RA like to seronegative spondyloarthritis (often HLA B
27 positive) was evaluated in CRD, Pune. This clinical
expression of CHIKV led the investigators to speculate
that CHIKV has a propensity to induce different types
of rheumatic disorders. An important concern from the
latter observation was whether ‘inflammatory arthritis’
following CHIKV was a frequent occurrence in the community.
A population based study was required and this was a basis
of the current CHIKV rural project. Village Bavi (District
Sholapur), 200 km from Pune (population size ~2200) on
the NH-4 highway to Sholapur was chosen as the study site.
A house-to-house survey of an adult population of 1450
was conducted. Cases with persistent RMSK post CHIKV illness
were followed up for 2 years till June 2008
In order to validate the observations of cases with persistent
RMSK beyond one year following CHIKV illness a neighboring
village (Modnimb, District Sholapur) population was selected;
Modnimb is 6 km from village Bavi and 155 km from Pune.
The Modnimb adult population (about 11000; the electoral
list contained 9672 names) was screened for cases suffering
from persistent RMSK following CHIKV illness, in December
2007.
As is known, and further shown by the data from this project,
the CHIKV arboviral illness is relatively benign and resolves
completely in over two thirds patients within one month.
Over 90% of the remaining one third cases that continue
to suffer from RMSK resolve within 16 weeks. At a community
level, <12% cases and <5% population continue to
suffer from RMSK for a year or so. More than 95% of the
latter cases at one year suffer from non-specific arthralgias
that need at its most symptomatic treatment, reassurance
and follow up. Less than 0.2% cases at one year suffer
from inflammatory arthritis which may be considered difficult
to treat and is relatively a serious form of RMSK that
can impact quality of life with a potential for physical
deformities.
Persistent RMSK was the principle objective of the CHIKV
project. The rural community data demonstrated that though
non specific RMSK pain and disorders are common following
CHIKV illness, inflammatory arthritis is an uncommon sequel.
A protocol driven program to compare oral chloroquin with
oral meloxicam (a standard non-steroidal anti-inflammatory
drug/NSAID) over 24 weeks of study period in patients
with moderately severe RMSK pain following CHIKV illness
was conducted.
This data showed that the predominant majority was relieved
within 16 weeks and few required long term symptomatic
care. At a community level, there was no evidence to prescribe
oral choloroquin or steroids in any form for post CHIKV
chronic RMSK, and symptomatic therapy with analgesics
(paracetamol) and/or NSAID (diclofenac, meloxicam) as
practiced in this study project, was sufficient.
List of Publications:
1. We presented our preliminary
results from village Bavi survey and the Pune rheumatology
referral outpatient during the proceedings of the national
conference on ‘Burden of rheumatic musculoskeletal
disorders in India’ in Pune on 14-15 Oct 06.
2. The preliminary observations
on the referral cohort of patients was presented at the
1st National Conference of Infectious Diseases, Mumbai
in 2007.
3. The Chikungunya (CHIK)
arthritis & rheumatism – an untold suffering.
Arthritis & Rheumatism (Abstract) September 2007;
Vol 56 9: 619-620.
4. Chikungunya virus aches
and pains: An emerging challenge
Arthritis & Rheumatism. 2008, Volume 58, Issue 9: 2921-2922.
5. Acute Chikungunya Profile
During The Indian Epidemic 2006 –Observation From
Village Bavi (Dist. Sholapur) Indian Journal of Rheumatology
2008 November Volume 3, Number 3 (Suppl); pp. S42
6. Chikungunya Related Persistent
Musculoskeletal (MSK) Profile Following The Indian Epidemic
2006 –Observations From Village Bavi (Dist.) Indian
Journal of Rheumatology 2008 November Volume 3, Number
3 (Suppl); pp. S42
7. Chronic aches and pains
following Chikungunya epidemic 2006 in Solapur (Maharashtra)
: Observations from Modnimb Arthritis camps. Journal of
Rheumatology 2008 November Volume 3, Number 3 (Suppl);
pp. S26
8. Does chloroquin work in
chikungunya related musculoskeletal (MSK) pain and arthropathy?
Results from the first community based controlled drug
trial. Indian Journal of Rheumatology 2008 November Volume
3, Number 3 (Suppl); pp. S26
|
|